
Kami sedia membantu
We are here to help
That was the slogan reiterated again and again by the Ministry of Health. We are expected to project altruism and willingness to serve the public, and expect nothing in return. As trained practitioners, we need not be told to do so, it has been ingrained in us since university.
It’s been more than 1 year since I joined civil service. I’ve enjoyed it at times, and reaped the benefits of being a civil servant (25 days of leave, not requiring to work weekends etc).
Your mileage may vary: every clinic/hospital has different staff and mentality. Public hospitals, in fact, are some of the best places. They employ the best and most motivated staff. They have a culture of excellence and quality control by specialists. They have state-of-the-art technology and facilities. The specialists generally have an air of quiet confidence and exert their supremacy through medical knowledge.
On the other hand, primary dental care clinics are overloaded with patients and paperwork. There is poor infrastructure, leaky roofs, fused bulbs and poor maintenance.

Oh and speaking of maintenance, most medical equipment in the ministry is serviced by Quantum Medical Solutions (QMS). There is a movement now to investigate the legitimacy of their tender to a contract of 13 years. Even staff in my clinic are claiming that QMS is a shady organisation used to siphon public money into pockets of the elite. Here’s an excerpt from change.org, I’ll leave it up to you to decide.
Quantum Medical Solutions also known as QMS, have been awarded a Tender of 13 years to supply and service the equipment of 2830 clinics over 10 states in Malaysia, where 1809 are Government Medical clinics and 1021 Government Dental Clinics.
I believe many healthcare professionals who has worked, managed or experienced the services rendered from QMS is not as promised.
Very frequently there seem to be a shortage or absence of equipment in clinics of desperate needs which are not met and thus service are interrupted/halted indefinitely. Whereas wastage of resources in purchasing items, equipments with exceptionally high value and not required are provided in what they term as “GAP LIST” under the MEET program which are not reviewed.
Kami sedia membantu. How to membantu when the facilities are in a sorry state?

My clinic in Gombak is a tiny clinic, but that’s not the problem. We have 2 dental chairs – one functioning, one broken. The broken one is used for extractions and checkups. The functioning one is for fillings and scaling. We don’t have a lab – so we don’t do dentures. X-ray machine is frequently broken, so we can’t do root canal treatments. These things are commissioned to be serviced by QMS, and time and time again after each repair it breaks down the next day. I can vouch firsthand for the petition above. It frustrates me and everyone else around me. But as civil servants, what can we do? Ideally, I hire an independent contractor to fix these things, and I can fire them if the quality is not what was expected. But I’m not in charge, nor are my bosses, we rely on funding from the bigwigs above and if nothing is changed, our clinic will remain 3rd world.
I’ve looked around and noticed that, as a consequence of poor infrastructure, the kami sedia membantu spirit has died away. Absolute altruism descended into relative nonchalance. The thing about practising in public sector is that many perceive treatment and advice to be relatively inconsequential. Patients generally are from the B40 segment of society and will adhere to what practitioners say. This is what’s called paternalism. In my years of training in the UK, paternalistic behaviour was frowned upon and could result in lawsuits.

That brings me to my last point: I’m not progressing my career here.
Day in day out, I feel sad, short-changed because I cannot offer my patients the care they deserve. My treatment options are limited to fillings, extractions and scaling. This is what’s called symptomatic treatment. I can’t do root canal treatments, crowns, dentures and more exciting stuff. Heck I can’t even take an X-ray to properly diagnose and treat.
The truth is this: this place is stifling my career growth as a dentist. As much as I am committed to altruism, to help the people of the world, I cannot continue to sit here and do nothing. I was told my wiser brother: “altruism [without adequate resources] is low-impact, more like grassroots activism.”
So I’ve decided to resign from the government and continue to pursue my career as a private dentist. With the civil service already so overstaffed and many more fresh grad dentists waiting patiently for their posting opportunity, I thought it might be a win-win for me to free myself of taxpayers’ burden as well as a vacancy for a fresh grad. By joining the private sector, I bear the hope that with better resources, I can give back to society by providing real solutions.



 Image source: Sensodyne
Image source: Sensodyne
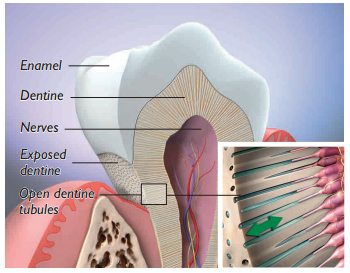 Image source
Image source
